Knee osteoarthritis (OA) is not only cartilage degeneration; it is strongly influenced by faulty biomechanics, abnormal loading, muscle imbalance, and poor lower-limb alignment.
During walking, standing, and stair climbing, the knee bears high loads. When alignment is disturbed, excessive stress falls on one compartment—most commonly the medial compartment—leading to cartilage wear, meniscal degeneration, pain, stiffness, and joint space narrowing.
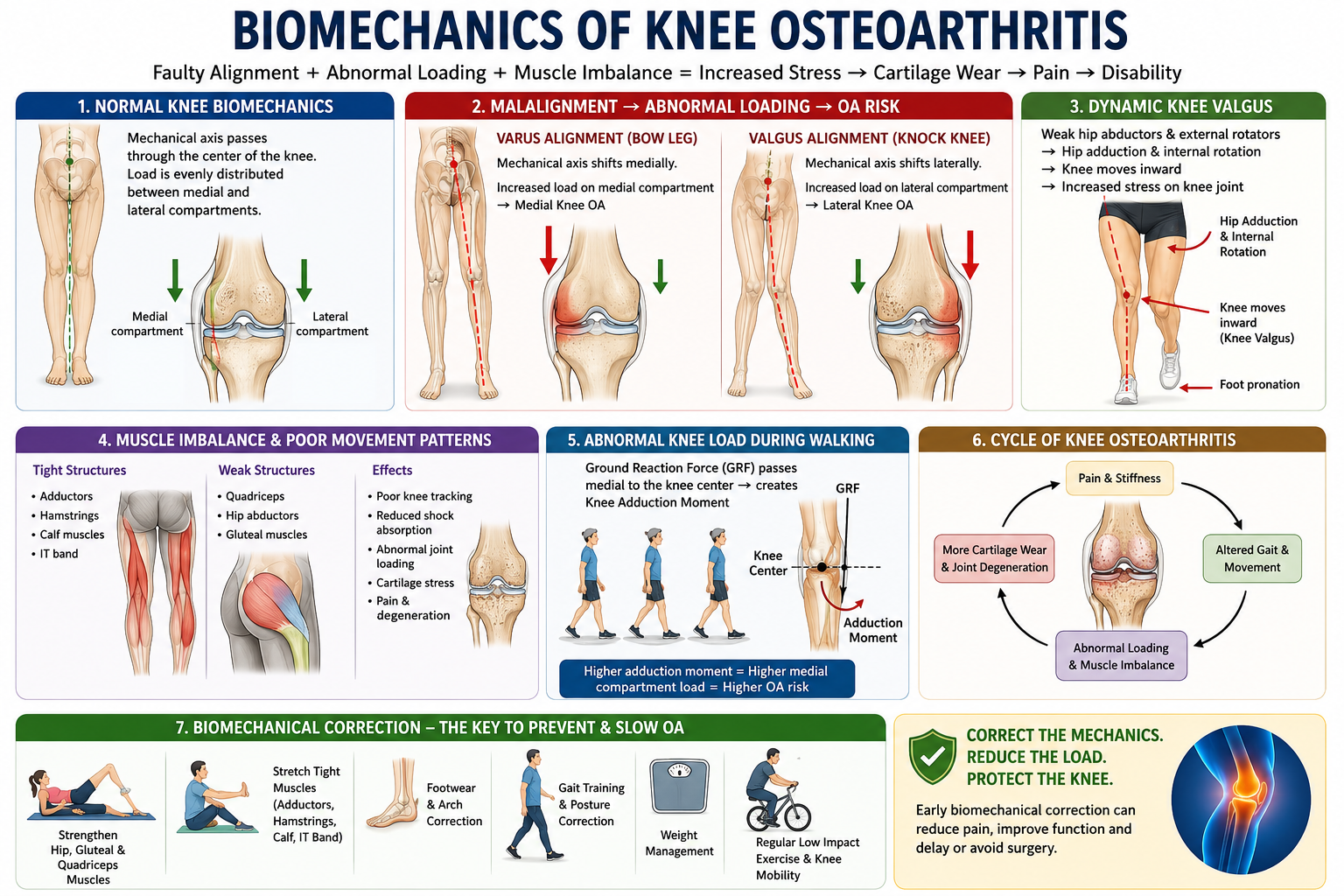
Key Biomechanical Factors
- Varus alignment increases medial compartment loading.
- Valgus alignment increases lateral compartment and patellofemoral stress.
- Weak hip abductors and external rotators allow excessive hip adduction and internal rotation, causing dynamic knee valgus.
- Flat foot or overpronation alters tibial rotation and increases knee stress.
- Tight adductors, hamstrings, calf muscles, and IT band disturb knee tracking and joint mechanics.
- Weak quadriceps and gluteal muscles reduce shock absorption and stability.
- Poor gait and reduced knee range of motion impair synovial fluid circulation and accelerate stiffness and degeneration.
Simple Patient Message
Knee OA is not just an age-related cartilage problem. In many patients, it worsens because the knee is being loaded incorrectly due to tight muscles, weak muscles, poor posture, flat feet, wrong footwear, obesity, and faulty walking patterns.
Early biomechanical correction can reduce pain, improve walking, decrease joint stress, protect cartilage, and slow OA progression.
Correction Measures
- Hip and gluteal strengthening
- Quadriceps strengthening
- Adductor, hamstring, calf, and IT band stretching
- Footwear and arch correction
- Gait training
- Posture correction
- Knee range-of-motion exercises
- Weight control
- Pain management, PRP, or visco-supplementation when clinically indicated
- Biomechanical correction
Correct the mechanics. Reduce the load. Protect the knee.